


This condition is more common in men. It manifests as pain and/or stiffness in the big toe. It can sometimes cause limping and difficulty wearing shoes. The shoe becomes uncomfortable to wear and causes friction against the bone.
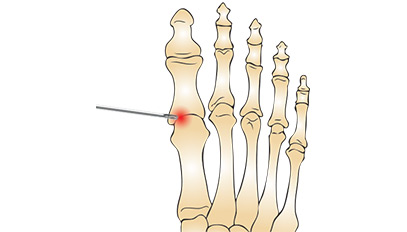
It's the formation of a neurologically derived swelling, 4 to 8 mm in diameter, originating from an interdigital plantar nerve located in the metatarsal space. Mechanically induced, neuroma is exacerbated by tight footwear and is more common in women. It may regress spontaneously.

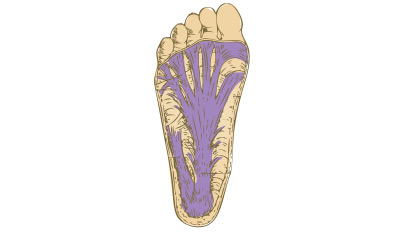
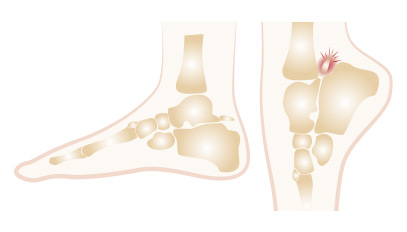
It is the largest and longest tendon in the body. Essential for walking, it has a propulsive effect and therefore must be very powerful. Also called the calcaneal tendon, it extends from the calf muscle and inserts into the calcaneus. It spans two joints: the knee and the ankle. It connects the triceps muscle to the heel.
It is a surgical procedure performed through percutaneous methods (2 to 3 puncture incisions), using an optic and camera to visualize the various compartments, thereby allowing a systematic exploration for diagnostic confirmation and therapeutic interventions.

It's a wound caused by a fragment of the nail penetrating the surrounding skin, which can vary in inflammation and infection levels, manifesting as redness, pain, and varying degrees of serous or purulent discharge. This condition commonly affects the big toe nail and can occur on the side or front of the nail.
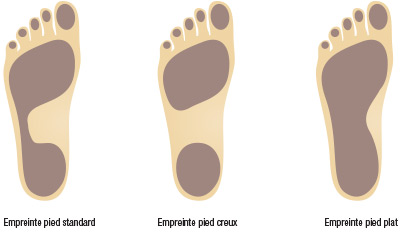
It's a foot with a widened footprint. Clinically, the inner arch is less pronounced, or even absent. Radiographic assessment shows normal axes, and in some advanced cases, there may be a misalignment of the bones of the first ray with the talus, the first cuneiform, and the navicular bone, with a downward collapse of the line on the profile.
Where multiple approaches create skin adhesions and stiffness,
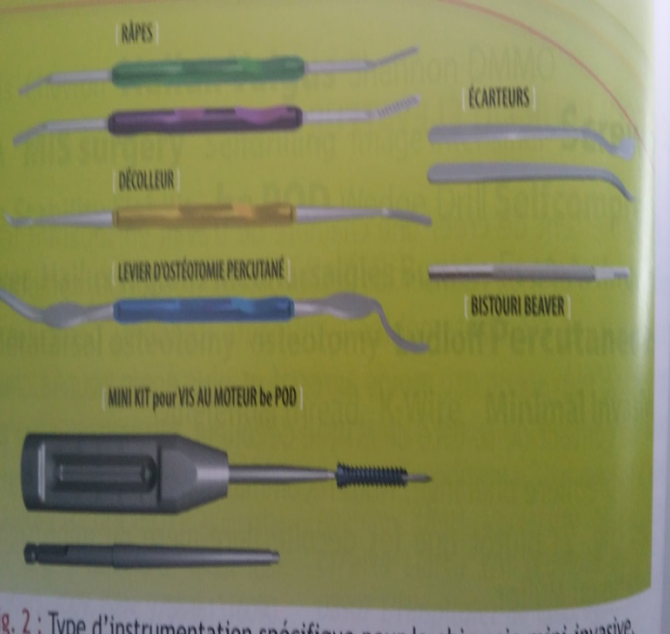
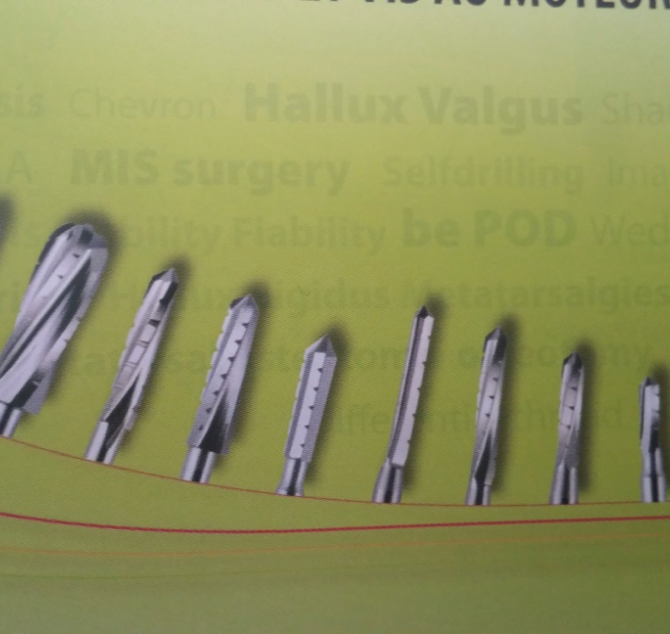
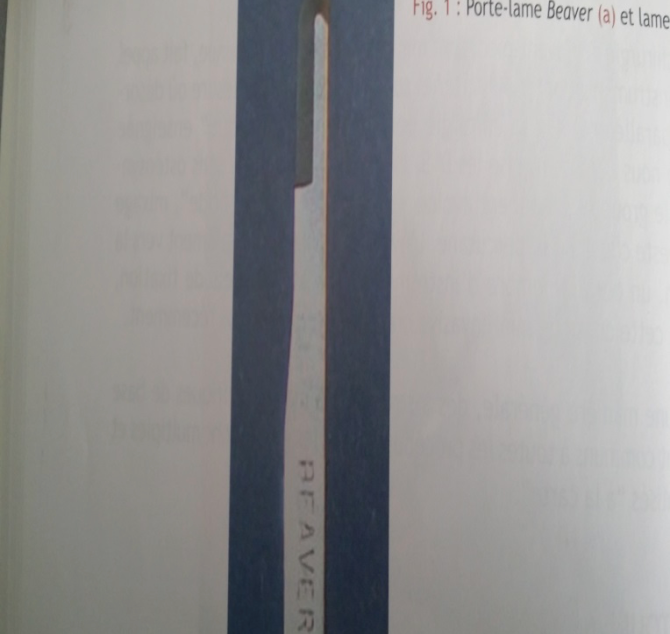
Percutaneous surgery brings real progress.
![]() The photo just after the operation.
The photo just after the operation.


Hallux Valgus and Index Minus
This article is intended for both patients and healthcare professionals. It focuses on the relationship between hallux valgus and index minus—two often-associated yet not always


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}