Hallux Rigidus & Hallux Limitus
affection of the big toe
Hallux rigidus and hallux limitus are common conditions affecting the big toe joint, leading to stiffness, pain, and limited motion. They can significantly impact daily activities and make it difficult to walk or wear shoes. Discover their main causes, symptoms, and available treatment options, including minimally invasive surgical techniques.

Diagnostic : Hallux Rigidus and Hallux Limitus
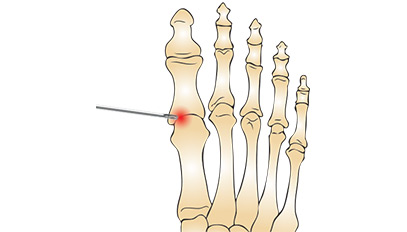
The diagnosis is made by an x-ray of the foot. This examination often reveals osteoarthritis of the metatarsophalangeal joint (MTP) of the big toe. When the deformity becomes advanced, a thickening of the skin (hyperkeratosis) is formed and a stiffness of the big toe is added, which can not bend upwards (fold) and cause pain and lameness.
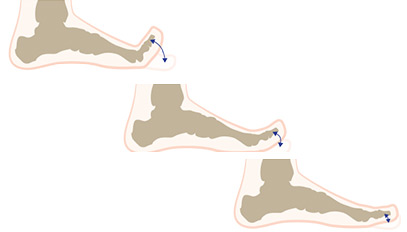
Avoidance Syndrome
To avoid pain, the patient dodges, unconsciously the support, and to avoid pain and lameness, involuntarily twists the foot outside on the outer edge of the foot, pressing more on the edge of the 5th metatarsal; It is the “avoidance syndrome”. One then walks the foot “turned” towards the outside, on the outer edge of the shoe.
Hallux Rigidus & Hallux Limitus Q & A
The treatment is primarily medical:
- NSAIDs (non-steroidal anti-inflammatory drugs) and analgesics (painkillers) in general, associated with local care and a modification of the footwear (wear a shoe half a size wider with rounded tip, flexible and wide).
- Wearing a sole is recommended. The latter will seek to raise the head of the first metatarsal.
This is recommended when the pain becomes disabling and when the medical treatment becomes inoperative. Several types of intervention can then be proposed.

Treatments that retain the mobility of the MTP joint
Consiste à enlever les ostéophytes et à libérer la capsule pour donner plus de mobilité. A faire aussi de la « toilette articulaire » qui consiste à éliminer les débris cartilagineux et fibrineux liés à l’arthrose. Ce geste étant souvent associé à une capsulotomie et/ou une arthrolyse.
By shortening the phalanx and / or the metatarsal (a few mm), the pressure on the joint is reduced and an amplitude of mobility is restored, if the cartilage is still preserved. This procedure alters the mechanics and can stabilize or slow down the development, which in the young patient leaves the possibility of an arthrodesis in a later phase, or a later age. This gesture is often associated with a capsulotomy and / or an arthrolysis.
Its indication is very limited; there is no product that has been the unanimity of the operators.
Treatment that blocks mobility
It is a procedure that consists of a suppression of the cartilage and a definitive fixation of the position of the phalanx with respect to the metatarsal. This intervention is radical, it suppresses pain. Its disadvantage is that it assumes a precise angle and therefore a precise height of the heel to be worn definitively, which can be very restrictive. In women, this must be explained in advance and a well-understood and fully agreed decision must be taken. This procedure can be performed in a closed, mini-invasive or open-hearth setting. In both cases, a fixation means is required: 2 cross screws or more solid with a plate osteosynthesis. (Arthrodesis with osteosynthesis per plate and screw)
Hallux Rigidus & Hallux Limitus: Terminology
Osteophites: bone formation around the joint, linked to the development of joint arthrosis. It is visible on the radio.
Exostose: Bony protrusion, at a distance from the joint, its formation is related to the excess friction of the bone against a rather rigid body, the shoe for example.
Osteotomy: section of the bone to straighten an axis, is done with a surgical saw, or by weakening the bone by perforations all around the bone, in a postage stamp making bone correction possible by a Simple manual tensioning effort. It is a sort of “fracture” for therapeutic purposes.
MTP joint: Metatarsophalangeal joint.
Arthrodesis: “definitive” blocking of a joint after resection of the cartilaginous surfaces, trailing an ankylosis: term meaning a loss of definitive movement of the said articulation.
First ray: the large toe essentially: Together the metatarsal and the 2 phalanges.
Inflammatory bursitis: serous, reddish, sometimes liquid fluid formation indicating mechanical friction.
Ulcerative bursitis: inflammatory bursitis with thinned skin that can ulcerate.
Horn: hard skin formation consisting of superficial epidermal tissue.
Hyperkeratosis: Applying keratin, which tends to strengthen the skin in the conflict in reaction to friction, it is a first sign of skin suffering, reflecting a mechanical cause.
Keratoma: Thick skin formation with early onset and sometimes medial perforation of somber color.
Capsulotomy: section of the joint capsule to release the joint.
Arthrolysis: release of the articulation and surrounding adherences with mobilization of the joint MTP.